General Information About Mycosis Fungoides and the Sézary Syndrome
Mycosis fungoides and the Sézary syndrome are diseases in which lymphocytes (a type of white blood cell) become malignant (cancerous) and affect the skin.
Normally, the bone marrow makes blood stem cells (immature cells) that become mature blood stem cells over time. A blood stem cell may become a myeloid stem cell or a lymphoid stem cell. A myeloid stem cell becomes a red blood cell, white blood cell, or platelet. A lymphoid stem cell becomes a lymphoblast and then one of three types of lymphocytes (white blood cells):
- B-cell lymphocytes that make antibodies to help fight infection.
- T-cell lymphocytes that help B-lymphocytes make the antibodies that help fight infection.
- Natural killer cells that attack cancer cells and viruses.
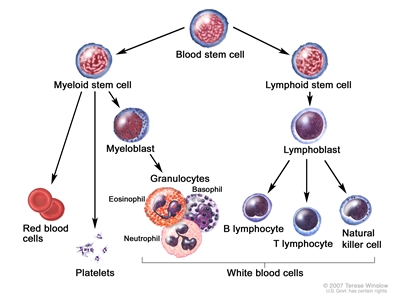
Blood cell development. A blood stem cell goes through several steps to become a red blood cell, platelet, or white blood cell.
In mycosis fungoides, T-cell lymphocytes become cancerous and affect the skin. In the Sézary syndrome, cancerous T-cell lymphocytes affect the skin and are in the blood.
Mycosis fungoides and the Sézary syndrome are types of cutaneous T-cell lymphoma.
Mycosis fungoides and the Sézary syndrome are the two most common types of cutaneous T-cell lymphoma (a type of non-Hodgkin lymphoma). For information about other types of skin cancer or non-Hodgkin lymphoma, see the following PDQ summaries:
- Adult Non-Hodgkin Lymphoma Treatment
- Skin Cancer Treatment
- Melanoma Treatment
- Kaposi Sarcoma Treatment
A sign of mycosis fungoides is a red rash on the skin.
Mycosis fungoides may go through the following phases:
- Premycotic phase: A scaly, red rash in areas of the body that usually are not exposed to the sun. This rash does not cause symptoms and may last for months or years. It is hard to diagnose the rash as mycosis fungoides during this phase.
- Patch phase: Thin, reddened, eczema -like rash.
- Plaque phase: Small raised bumps (papules) or hardened lesions on the skin, which may be reddened.
- Tumor phase: Tumors form on the skin. These tumors may develop ulcers and the skin may get infected.
Check with your doctor if you have any of these signs.
In the Sézary syndrome, cancerous T-cells are found in the blood.
Also, skin all over the body is reddened, itchy, peeling, and painful. There may also be patches, plaques, or tumors on the skin. It is not known if the Sézary syndrome is an advanced form of mycosis fungoides or a separate disease.
Tests that examine the skin and blood are used to detect (find) and diagnose mycosis fungoides and the Sézary syndrome.
The following tests and procedures may be used:
- Physical exam and history: An exam of the body to check general signs of health, including checking for signs of disease, such as lumps, the number and type of skin lesions, or anything else that seems unusual. Pictures of the skin and a history of the patient's health habits and past illnesses and treatments will also be taken.
- Complete blood count with differential: A procedure in which a sample of blood is drawn and checked for the following:
- The number of red blood cells and platelets.
- The number and type of white blood cells.
- The amount of hemoglobin (the protein that carries oxygen) in the red blood cells.
- The portion of the blood sample made up of red blood cells.
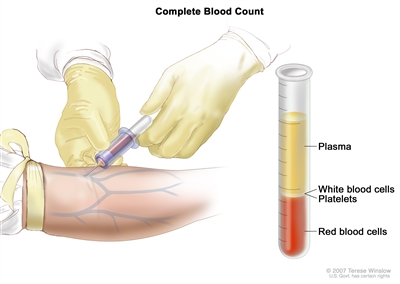
Complete blood count (CBC). Blood is collected by inserting a needle into a vein and allowing the blood to flow into a tube. The blood sample is sent to the laboratory and the red blood cells, white blood cells, and platelets are counted. The CBC is used to test for, diagnose, and monitor many different conditions. - Peripheral blood smear: A procedure in which a sample of blood is viewed under a microscope to count different circulating blood cells (red blood cells, white blood cells, platelets, etc.) and see whether the cells look normal.
- Skin biopsy: The removal of cells or tissues so they can be viewed under a microscope to check for signs of cancer. The doctor may remove a growth from the skin, which will be examined by a pathologist. More than one skin biopsy may be needed to diagnose mycosis fungoides.
- Immunophenotyping: A process used to identify cells, based on the types of antigens or markers on the surface of the cell. This process may include special staining of the blood cells. It is used to diagnose specific types of leukemia and lymphoma by comparing the cancer cells to normal cells of the immune system.
- T-cell receptor (TCR) gene rearrangement test: A laboratory test in which cells in a sample of tissue are checked to see if there is a certain change in the genes. This gene change can lead to too many of one kind of T-cells (white blood cells that fight infection) to be made.
- Flow cytometry: A laboratory test that measures the number of cells in a sample of blood, the percentage of live cells in a sample, and certain characteristics of cells, such as size, shape, and the presence of tumor markers on the cell surface. The cells are stained with a light-sensitive dye, placed in a fluid, and passed in a stream before a laser or other type of light. The measurements are based on how the light-sensitive dye reacts to the light.
Certain factors affect prognosis (chance of recovery) and treatment options.
The prognosis (chance of recovery) and treatment options depend on the following:
- The stage of the cancer.
- The type of lesion (patches, plaques, or tumors).
Mycosis fungoides and the Sézary syndrome are hard to cure. Treatment is usually palliative, to relieve symptoms and improve the quality of life. Patients with early stage disease may live many years.
Stages of Mycosis Fungoides and the Sézary Syndrome
After mycosis fungoides and the Sézary syndrome have been diagnosed, tests are done to find out if cancer cells have spread from the skin to other parts of the body.
The process used to find out if cancer has spread from the skin to other parts of the body is called staging. The information gathered from the staging process determines the stage of the disease. It is important to know the stage in order to plan treatment.
The following procedures may be used in the staging process:
- Chest x-ray: An x-ray of the organs and bones inside the chest. An x-ray is a type of energy beam that can go through the body and onto film, making a picture of areas inside the body.
- CT scan (CAT scan): A procedure that makes a series of detailed pictures of areas inside the body, such as the lymph nodes, chest, abdomen, and pelvis, taken from different angles. The pictures are made by a computer linked to an x-ray machine. A dye may be injected into a vein or swallowed to help the organs or tissues show up more clearly. This procedure is also called computed tomography, computerized tomography, or computerized axial tomography.
- PET scan (positron emission tomography scan): A procedure to find malignant tumor cells in the body. A small amount of radioactive glucose (sugar) is injected into a vein. The PET scanner rotates around the body and makes a picture of where glucose is being used in the body. Malignant tumor cells show up brighter in the picture because they are more active and take up more glucose than normal cells do.
- Lymph node biopsy: The removal of all or part of a lymph node. A pathologist views the tissue under a microscope to look for cancer cells.
- Bone marrow aspiration and biopsy: The removal of bone marrow and a small piece of bone by inserting a hollow needle into the hipbone or breastbone. A pathologist views the bone marrow and bone under a microscope to look for signs of cancer.
There are three ways that cancer spreads in the body.
Cancer can spread through tissue, the lymph system, and the blood:
- Tissue. The cancer spreads from where it began by growing into nearby areas.
- Lymph system. The cancer spreads from where it began by getting into the lymph system. The cancer travels through the lymph vessels to other parts of the body.
- Blood. The cancer spreads from where it began by getting into the blood. The cancer travels through the blood vessels to other parts of the body.
Cancer may spread from where it began to other parts of the body.
When cancer spreads to another part of the body, it is called metastasis. Cancer cells break away from where they began (the primary tumor) and travel through the lymph system or blood.
- Lymph system. The cancer gets into the lymph system, travels through the lymph vessels, and forms a tumor (metastatic tumor) in another part of the body.
- Blood. The cancer gets into the blood, travels through the blood vessels, and forms a tumor (metastatic tumor) in another part of the body.
The metastatic tumor is the same type of cancer as the primary tumor. For example, if mycosis fungoides spreads to the liver, the cancer cells in the liver are actually mycosis fungoides cells. The disease is metastatic mycosis fungoides, not liver cancer.
The following stages are used for mycosis fungoides and the Sézary syndrome:
Stage I Mycosis Fungoides
Stage I is divided into stage IA and stage IB as follows:
- Stage IA: Less than 10% of the skin surface is covered with patches, papules, and/or plaques.
- Stage IB: Ten percent or more of the skin surface is covered with patches, papules, and/or plaques.
There may be abnormal lymphocytes in the blood but they are not cancerous.
Stage II Mycosis Fungoides
Stage II is divided into stage IIA and stage IIB as follows:
- Stage IIA: Any amount of the skin surface is covered with patches, papules, and/or plaques. Lymph nodes are enlarged but cancer has not spread to them.
- Stage IIB: One or more tumors that are 1 centimeter or larger are found on the skin. Lymph nodes may be enlarged but cancer has not spread to them.
There may be abnormal lymphocytes in the blood but they are not cancerous.
Stage III Mycosis Fungoides
In stage III, nearly all of the skin is reddened and may have patches, papules, plaques, or tumors. Lymph nodes may be enlarged but cancer has not spread to them.
There may be abnormal lymphocytes in the blood but they are not cancerous.
Stage IV Mycosis Fungoides
Stage IV is divided into stage IVA and stage IVB as follows:
- Stage IVA: Most of the skin is reddened and any amount of the skin surface is covered with patches, papules, plaques, or tumors, and either:
- cancer has spread to lymph nodes and there may be cancerous lymphocytes in the blood; or
- there are cancerous lymphocytes in the blood and lymph nodes may be enlarged, but cancer has not spread to them.
- Stage IVB: Most of the skin is reddened and any amount of the skin surface is covered with patches, papules, plaques, or tumors. Cancer has spread to other organs in the body. Lymph nodes may be enlarged and cancer may have spread to them. There may be cancerous lymphocytes in the blood.
Stage IV Sézary Syndrome
In stage IV:
- Most of the skin is reddened and covered with patches, papules, plaques, or tumors; and
- There is a high level of cancerous lymphocytes in the blood; and
- Lymph nodes may be enlarged and cancer may have spread to them.
Recurrent Mycosis Fungoides and the Sézary Syndrome
Recurrent mycosis fungoides and the Sézary syndrome are cancers that have recurred (come back) after they have been treated. The cancer may come back in the skin or in other parts of the body.
Treatment Option Overview
There are different types of treatment for patients with mycosis fungoides and the Sézary syndrome cancer.
Different types of treatment are available for patients with mycosis fungoides and the Sézary syndrome. Some treatments are standard (the currently used treatment), and some are being tested in clinical trials. A treatment clinical trial is a research study meant to help improve current treatments or obtain information on new treatments for patients with cancer. When clinical trials show that a new treatment is better than the standard treatment, the new treatment may become the standard treatment. Patients may want to think about taking part in a clinical trial. Some clinical trials are open only to patients who have not started treatment.
Six types of standard treatment are used:
Photodynamic therapy
Photodynamic therapy is a cancer treatment that uses a drug and a certain type of laser light to kill cancer cells. A drug that is not active until it is exposed to light is injected into a vein. The drug collects more in cancer cells than in normal cells. For skin cancer, laser light is shined onto the skin and the drug becomes active and kills the cancer cells. Photodynamic therapy causes little damage to healthy tissue. Patients undergoing photodynamic therapy will need to limit the amount of time spent in sunlight.
In one type of photodynamic therapy, called psoralen and ultraviolet A (PUVA) therapy, the patient receives a drug called psoralen and then ultraviolet radiation is directed to the skin. In another type of photodynamic therapy, called extracorporeal photochemotherapy, the patient is given drugs and then some blood cells are taken from the body, put under a special ultraviolet A light, and put back into the body.
Radiation therapy
Radiation therapy is a cancer treatment that uses high-energy x-rays or other types of radiation to kill cancer cells or keep them from growing. There are two types of radiation therapy:
- External radiation therapy uses a machine outside the body to send radiation toward the cancer.
- Internal radiation therapy uses a radioactive substance sealed in needles, seeds, wires, or catheters that are placed directly into or near the cancer.
The way the radiation therapy is given depends on the type and stage of the cancer being treated. External radiation therapy is used to treat mycosis fungoides and the Sézary syndrome, and may also be used as palliative therapy to relieve symptoms and improve quality of life. Sometimes, total skin electron beam (TSEB) radiation therapy is used to treat mycosis fungoides and the Sézary syndrome. This is a type of external radiation treatment in which a radiation therapy machine aims electrons (tiny, invisible particles) at the skin covering the whole body.
Ultraviolet B (UVB) radiation therapy uses a special lamp or laser that directs UVB radiation at the skin.
Chemotherapy
Chemotherapy is a cancer treatment that uses drugs to stop the growth of cancer cells, either by killing the cells or by stopping them from dividing. When chemotherapy is taken by mouth or injected into a vein or muscle, the drugs enter the bloodstream and can reach cancer cells throughout the body (systemic chemotherapy). When chemotherapy is placed directly into the cerebrospinal fluid, an organ, or a body cavity such as the abdomen, the drugs mainly affect cancer cells in those areas (regional chemotherapy). Sometimes the chemotherapy is topical (put on the skin in a cream, lotion, or ointment). The way the chemotherapy is given depends on the type and stage of the cancer being treated.
See Drugs Approved for Non-Hodgkin Lymphoma for more information. (Mycosis fungoides and the Sézary syndrome are types of non-Hodgkin lymphoma.)
Other drug therapy
Topical corticosteroids are used to relieve red, swollen, and inflamed skin. They are a type of steroid. Topical corticosteroids may be in a cream, lotion, or ointment.
Retinoids, such as bexarotene, are drugs related to vitamin A that can slow the growth of certain types of cancer cells. The retinoids may be taken by mouth or put on the skin.
See Drugs Approved for Non-Hodgkin Lymphoma for more information. (Mycosis fungoides and the Sézary syndrome are types of non-Hodgkin lymphoma.)
Biologic therapy
Biologic therapy is a treatment that uses the patient's immune system to fight cancer. Substances made by the body or made in a laboratory are used to boost, direct, or restore the body's natural defenses against cancer. This type of cancer treatment is also called biotherapy or immunotherapy.
Interferon is a type of biologic therapy used to treat mycosis fungoides and the Sézary syndrome. It interferes with the division of cancer cells and can slow tumor growth.
See Drugs Approved for Non-Hodgkin Lymphoma for more information. (Mycosis fungoides and the Sézary syndrome are types of non-Hodgkin lymphoma.)
Targeted therapy
Targeted therapy is a treatment that uses drugs or other substances to identify and attack specific cancer cells without harming normal cells. Monoclonal antibody therapy and other types of targeted therapies are used to treat mycosis fungoides and the Sézary syndrome.
Alemtuzumab is a monoclonal antibody used to treat mycosis fungoides and the Sézary syndrome. Monoclonal antibody therapy uses antibodies made in the laboratory, from a single type of immune system cell. These antibodies can identify substances on cancer cells or normal substances that may help cancer cells grow. The antibodies attach to the substances and kill the cancer cells, block their growth, or keep them from spreading. Monoclonal antibodies are given by infusion. They may be used alone or to carry drugs, toxins, or radioactive material directly to cancer cells.
Other types of monoclonal antibody therapy are being studied in clinical trials to treat mycosis fungoides and the Sézary syndrome.
Vorinostat and romidepsin are two of the histone deacetylase (HDAC) inhibitors used to treat mycosis fungoides and the Sézary syndrome. HDAC inhibitors cause a chemical change that stops tumor cells from dividing.
Pralatrexate is a dihydrofolate reductase (DHFR) inhibitor used to treat mycosis fungoides and the Sézary syndrome. It builds up in cancer cells and stops them from using folate, a nutrient needed for cells to divide. Pralatrexate may slow the growth of tumors and kill cancer cells.
See Drugs Approved for Non-Hodgkin Lymphoma for more information. (Mycosis fungoides and the Sézary syndrome are types of non-Hodgkin lymphoma.)
New types of treatment are being tested in clinical trials.
This summary section describes treatments that are being studied in clinical trials. It may not mention every new treatment being studied. Information about clinical trials is available from the NCI website.
High-dose chemotherapy and radiation therapy with stem cell transplant
This treatment is a method of giving high doses of chemotherapy and radiation therapy and replacing blood-forming cells destroyed by the cancer treatment. Stem cells (immature blood cells) are removed from the bone marrow or blood of the patient or a donor and are frozen and stored. After therapy is completed, the stored stem cells are thawed and given back to the patient through an infusion. These reinfused stem cells grow into (and restore) the body's blood cells.
Patients may want to think about taking part in a clinical trial.
For some patients, taking part in a clinical trial may be the best treatment choice. Clinical trials are part of the cancer research process. Clinical trials are done to find out if new cancer treatments are safe and effective or better than the standard treatment.
Many of today's standard treatments for cancer are based on earlier clinical trials. Patients who take part in a clinical trial may receive the standard treatment or be among the first to receive a new treatment.
Patients who take part in clinical trials also help improve the way cancer will be treated in the future. Even when clinical trials do not lead to effective new treatments, they often answer important questions and help move research forward.
Patients can enter clinical trials before, during, or after starting their cancer treatment.
Some clinical trials only include patients who have not yet received treatment. Other trials test treatments for patients whose cancer has not gotten better. There are also clinical trials that test new ways to stop cancer from recurring (coming back) or reduce the side effects of cancer treatment.
Clinical trials are taking place in many parts of the country. See the Treatment Options section that follows for links to current treatment clinical trials. These have been retrieved from NCI's listing of clinical trials.
Follow-up tests may be needed.
Some of the tests that were done to diagnose the cancer or to find out the stage of the cancer may be repeated. Some tests will be repeated in order to see how well the treatment is working. Decisions about whether to continue, change, or stop treatment may be based on the results of these tests.
Some of the tests will continue to be done from time to time after treatment has ended. The results of these tests can show if your condition has changed or if the cancer has recurred (come back). These tests are sometimes called follow-up tests or check-ups.
Treatment Options by Stage
Stage I Mycosis Fungoides
Treatment of stage I mycosis fungoides may include the following:
- PUVA therapy. Biologic therapy may also be given.
- Radiation therapy. In some cases, radiation therapy is given to skin lesions, as palliative therapy to reduce tumor size or relieve symptoms and improve quality of life.
- Topical corticosteroid therapy.
- Retinoid therapy.
- Topical or systemic chemotherapy.
- Biologic therapy. Topical chemotherapy may also be given.
- Targeted therapy.
- A clinical trial of a new treatment.
Check the list of NCI-supported cancer clinical trials that are now accepting patients with stage I mycosis fungoides/Sezary syndrome. For more specific results, refine the search by using other search features, such as the location of the trial, the type of treatment, or the name of the drug. Talk with your doctor about clinical trials that may be right for you. General information about clinical trials is available from the NCI website.
Stage II Mycosis Fungoides
Treatment of stage II mycosis fungoides is palliative (to relieve symptoms and improve the quality of life) and may include the following:
- PUVA therapy. Biologic therapy may also be given.
- Radiation therapy.
- Topical corticosteroid therapy.
- Retinoid therapy.
- Topical or systemic chemotherapy.
- Biologic therapy. Topical chemotherapy may also be given.
- Targeted therapy.
- A clinical trial of a new treatment.
Check the list of NCI-supported cancer clinical trials that are now accepting patients with stage II mycosis fungoides/Sezary syndrome. For more specific results, refine the search by using other search features, such as the location of the trial, the type of treatment, or the name of the drug. Talk with your doctor about clinical trials that may be right for you. General information about clinical trials is available from the NCI website.
Stage III Mycosis Fungoides
Treatment of stage III mycosis fungoides is palliative (to relieve symptoms and improve the quality of life) and may include the following:
- PUVA therapy. Systemic chemotherapy or biologic therapy may also be given.
- Extracorporeal photochemotherapy.
- Radiation therapy.
- Topical corticosteroid therapy.
- Retinoid therapy.
- Systemic chemotherapy with one or more drugs. Topical chemotherapy or radiation therapy may also be given.
- Topical chemotherapy.
- Biologic therapy. Topical chemotherapy may also be given.
- Targeted therapy.
- A clinical trial of a new treatment.
Check the list of NCI-supported cancer clinical trials that are now accepting patients with stage III mycosis fungoides/Sezary syndrome. For more specific results, refine the search by using other search features, such as the location of the trial, the type of treatment, or the name of the drug. Talk with your doctor about clinical trials that may be right for you. General information about clinical trials is available from the NCI website.
Stage IV Mycosis Fungoides and the Sézary Syndrome
Treatment of stage IV mycosis fungoides and stage IV Sézary syndrome is palliative (to relieve symptoms and improve the quality of life) and may include the following:
- PUVA therapy. Systemic chemotherapy or biologic therapy may also be given.
- Extracorporeal photochemotherapy. Radiation therapy may also be given.
- Radiation therapy.
- Topical corticosteroid therapy.
- Retinoid therapy.
- Systemic chemotherapy with one or more drugs, or topical chemotherapy.
- Biologic therapy. Topical chemotherapy may also be given.
- Targeted therapy.
- A clinical trial of a new treatment.
Check the list of NCI-supported cancer clinical trials that are now accepting patients with stage IV mycosis fungoides/Sezary syndrome. For more specific results, refine the search by using other search features, such as the location of the trial, the type of treatment, or the name of the drug. Talk with your doctor about clinical trials that may be right for you. General information about clinical trials is available from the NCI website.
Treatment Options for Recurrent Mycosis Fungoides and the Sézary Syndrome
Treatment of recurrent mycosis fungoides and the Sézary syndrome is usually within a clinical trial and may include the following:
- PUVA therapy with biologic therapy.
- Extracorporeal photochemotherapy.
- Repeat treatment with radiation therapy.
- Retinoid therapy.
- Systemic chemotherapy.
- Biologic therapy.
- Targeted therapy.
- High-dose chemotherapy with stem cell transplant.
- Topical chemotherapy or PUVA therapy to relieve symptoms and improve the quality of life.
- Topical corticosteroid therapy, to relieve symptoms and improve the quality of life.
Check the list of NCI-supported cancer clinical trials that are now accepting patients with recurrent mycosis fungoides/Sezary syndrome. For more specific results, refine the search by using other search features, such as the location of the trial, the type of treatment, or the name of the drug. Talk with your doctor about clinical trials that may be right for you. General information about clinical trials is available from the NCI website.
To Learn More About Mycosis Fungoides and the Sézary Syndrome
For more information from the National Cancer Institute about mycosis fungoides and the Sézary syndrome, see the following:
- Lymphoma Home Page
- Photodynamic Therapy for Cancer
- Drugs Approved for Non-Hodgkin Lymphoma
- Biological Therapies for Cancer
- Targeted Cancer Therapies
For general cancer information and other resources from the National Cancer Institute, see the following:
- About Cancer
- Staging
- Chemotherapy and You: Support for People With Cancer
- Radiation Therapy and You: Support for People With Cancer
- Coping with Cancer
- Questions to Ask Your Doctor about Cancer
- For Survivors and Caregivers
About This PDQ Summary
About PDQ
Physician Data Query (PDQ) is the National Cancer Institute's (NCI's) comprehensive cancer information database. The PDQ database contains summaries of the latest published information on cancer prevention, detection, genetics, treatment, supportive care, and complementary and alternative medicine. Most summaries come in two versions. The health professional versions have detailed information written in technical language. The patient versions are written in easy-to-understand, nontechnical language. Both versions have cancer information that is accurate and up to date and most versions are also available in Spanish.
PDQ is a service of the NCI. The NCI is part of the National Institutes of Health (NIH). NIH is the federal government's center of biomedical research. The PDQ summaries are based on an independent review of the medical literature. They are not policy statements of the NCI or the NIH.
Purpose of This Summary
This PDQ cancer information summary has current information about the treatment of mycosis fungoides and the Sézary Syndrome. It is meant to inform and help patients, families, and caregivers. It does not give formal guidelines or recommendations for making decisions about health care.
Reviewers and Updates
Editorial Boards write the PDQ cancer information summaries and keep them up to date. These Boards are made up of experts in cancer treatment and other specialties related to cancer. The summaries are reviewed regularly and changes are made when there is new information. The date on each summary ("Date Last Modified") is the date of the most recent change.
The information in this patient summary was taken from the health professional version, which is reviewed regularly and updated as needed, by the PDQ Adult Treatment Editorial Board.
Clinical Trial Information
A clinical trial is a study to answer a scientific question, such as whether one treatment is better than another. Trials are based on past studies and what has been learned in the laboratory. Each trial answers certain scientific questions in order to find new and better ways to help cancer patients. During treatment clinical trials, information is collected about the effects of a new treatment and how well it works. If a clinical trial shows that a new treatment is better than one currently being used, the new treatment may become "standard." Patients may want to think about taking part in a clinical trial. Some clinical trials are open only to patients who have not started treatment.
Clinical trials are listed in PDQ and can be found online at NCI's website. Many cancer doctors who take part in clinical trials are also listed in PDQ. For more information, call the Cancer Information Service 1-800-4-CANCER (1-800-422-6237).
Permission to Use This Summary
PDQ is a registered trademark. The content of PDQ documents can be used freely as text. It cannot be identified as an NCI PDQ cancer information summary unless the whole summary is shown and it is updated regularly. However, a user would be allowed to write a sentence such as "NCI's PDQ cancer information summary about breast cancer prevention states the risks in the following way: [include excerpt from the summary]."
The best way to cite this PDQ summary is:
PDQ® Adult Treatment Editorial Board. PDQ Mycosis Fungoides and the Sézary Syndrome Treatment. Bethesda, MD: National Cancer Institute. Updated <MM/DD/YYYY>. Available at: https://www.cancer.gov/types/lymphoma/patient/mycosis-fungoides-treatment-pdq. Accessed <MM/DD/YYYY>. [PMID: 26389317]
Images in this summary are used with permission of the author(s), artist, and/or publisher for use in the PDQ summaries only. If you want to use an image from a PDQ summary and you are not using the whole summary, you must get permission from the owner. It cannot be given by the National Cancer Institute. Information about using the images in this summary, along with many other images related to cancer can be found in Visuals Online. Visuals Online is a collection of more than 2,000 scientific images.
Disclaimer
The information in these summaries should not be used to make decisions about insurance reimbursement. More information on insurance coverage is available on Cancer.gov on the Managing Cancer Care page.
Contact Us
More information about contacting us or receiving help with the Cancer.gov website can be found on our Contact Us for Help page. Questions can also be submitted to Cancer.gov through the website's E-mail Us.
Last Revised: 2016-07-22
If you want to know more about cancer and how it is treated, or if you wish to know about clinical trials for your type of cancer, you can call the NCI's Cancer Information Service at 1-800-422-6237, toll free. A trained information specialist can talk with you and answer your questions.